Quantitative Fluorescent PCR is a PCR-based technique in which a low number of PCR cycles are used, such that the endpoint of the reaction reflects the DNA or chromosome copy number in the test sample.
There are two key steps to QF-PCR, amplification and quantification. Firstly, specific regions of DNA are amplified. And then secondly, the amount of DNA present in those regions is quantified.
We will first concentrate on the initial QF-PCR step, the amplification of DNA. QF-PCR exploits DNA regions containing specific DNA markers or Short Tandem Repeats, or STRs for short, that are scattered throughout the genome.

These STRs are repeat sequences of tetranucleotides, or four bases, and are highly polymorphic in terms of their number of repeats, so that and individual is highly likely to have a different number of repeats on each homologue. Primers are designed for each marker. These primers are labelled with a fluorescent tag. The repeats are then amplified by PCR, allowing comparison of the relative dosages of maternal and paternal chromosome and against those of a normal control. Only those STRs or markers that differ from each other are chosen for analysis, so-called informative markers. The example here shows an STR which has six repeats on the maternal chromosome 21 and four repeats on the paternal chromosome 21, and is therefore informative.

The marker regions are amplified in a PCR reaction. However, there is a very important difference in the PCR reaction used for QF-PCR. That is, that the reaction is stopped early in the exponential phase, generally between 24 and 26 cycles. This is because the assumption is that within the early exponential of amplification, the amount of product present is directly proportional to the amount of target sequence present in the original template. Therefore, the results indicate the quantity of original template present. The success of the assay is therefore dependent on the amount of DNA used in relation to the number of amplification cycles.
The second part of the QF-PCR experiment involves quantification of the DNA.

In this phase, the PCR products are separated by capillary electrophoresis. Lasers excite the fluorochromes, and the relative amount of fluorescence emitted, which is proportional to the amount of each amplified allele present, is measured.
QF-PCR is used to confirm copy number variants detected by array CGH, MLPA, or Next-Generation Sequencing read depth analysis.

However, one of its primary uses, given the speed of results and associated low cost, is in prenatal aneuploidy testing. We will focus on this use of QF-PCR for the remainder of this presentation.
Prenatal aneuploidy testing can be undertaken on CVS or amniotic fluid samples. It has a fast turnaround time, and the result is available within three to five days.

Analysis is done on markers from chromosomes 13, 18, and 21, and may also be done on markers from the sex chromosomes. This diagram shows a series of markers across chromosomes 13, 18, and 21 that are used for aneuploidy testing. The blue markers are the primary markers, which are analysed first. And the red markers are additional markers, which can be used for confirmation of a result, or if the primary markers are uninformative. A pair of primers is designed for each STR to be run, and multiple pairs of primers can be run in a single reaction. In this way, multiple loci are screened across multiple chromosomes simultaneously.
Analysis is done on markers from chromosomes 13, 18, and 21, and may also be done on markers from the sex chromosomes.

This diagram shows a series of markers across chromosomes 13, 18, and 21 that are used for aneuploidy testing. The blue markers are the primary markers, which are analysed first. And the red markers are additional markers, which can be used for confirmation of a result, or if the primary markers are uninformative. A pair of primers is designed for each STR to be run, and multiple pairs of primers can be run in a single reaction. In this way, multiple loci are screened across multiple chromosomes simultaneously.

Markers can also be used across the X and Y chromosomes to check the sex chromosome complement. Analysis software is used to compare peak heights between different alleles of each STR.

The left-hand diagram shows a normal diallelic sample, that is representing markers from two chromosomes. The top marker is homozygous in this sample, giving only one big peak, which is uninformative. The marker below is heterozygous, and in this normal sample gives a 1:1 ratio. The right-hand diagram shows a triallelic sample, resulting from trisomy. Again, the top marker is uninformative, as all three alleles have the same length STR.
The middle marker shows two peaks in an abnormal 2:1 ratio, reflecting the presence of two copies of one of the parental alleles. The bottom marker shows an abnormal triallelic result of 1:1:1. This reflects the presence of three different parental alleles, likely to have resulted from meiotic nondisjunction during oogenesis. 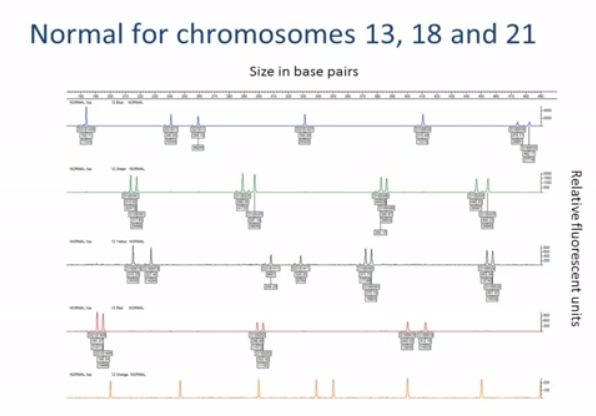

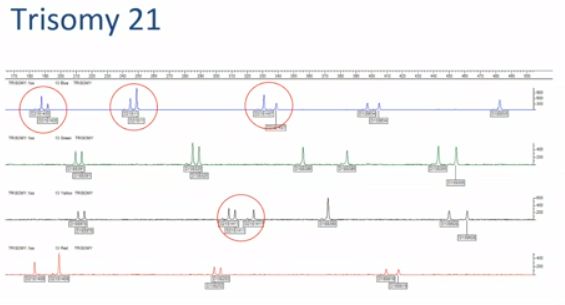
Results from multiple markers are represented graphically for analysis. The ratios are then also displayed in an Excel spreadsheet. This graph shows the result from a sample that is normal for chromosomes 13, 18, and 21. In the blue trace, you can see some uninformative homozygous markers, giving just a single peak. In the green, black, and red traces, you can see that the marker peaks are paired,and their heights are in a normal 1:1 ratio. This graph shows a sample with trisomy 21.

Here, you can see that the chromosome 21 markers, ringed, are present in abnormal 2:1 or 1:1:1 ratios. The other markers, for chromosomes 18 and 13, are present in normal 1:1 ratios.
This result shows mosaicism for trisomy 18. The boxed peaks are the chromosome 18 markers. Most of them appear normal, but if you look carefully at the boxed peaks on the top blue trace, you can see a small third peak in the middle. This subtle change indicates the presence of a third allele at this chromosome 18 marker. The level of mosaicism in this sample is around 15%, which is usually the minimum limit of detection. As with all prenatal samples, especially CVS samples, confined placental mosaicism can be a problem. A triallelic result indicates the meiotic nondisjunction event during oogenesis, so carries a high risk of foetal involvement.
However, a diallelic result when none of the markers confirm nondisjunction raises the possibility that the cell line may be confined to the placenta. In all cases, the QF-PCR result should be carefully interpreted in conjunction with the ultrasound findings. Any abnormal results on CVS are further investigated with a karyotype, and further testing with amniocentesis is often undertaken if the CVS results are ambiguous.

Maternal cell contamination is a common problem with prenatal samples. It is detectable by skewed ratios or extra peaks involving all the chromosomes, as shown here. This sample was reported as unsuitable on the basis of the evident maternal cell contamination. In summary, QF-PCR involves the amplification and quantification of markers on chromosomes of interest.
QF-PCR is used to confirm copy number variants detected by other methods. However, its main application is in prenatal aneuploidy testing as it is a quick, reliable, and cost-effective test.
Source:-


No comments:
Post a Comment